-
ขนาดตัวอักษร
 |
|
 |
|
 |
|

แอลกอฮอล์ กรณีตัวอย่าง ผู้ป่วยแอลกอฮอล์ ชายไทยคู่ อายุ 35 ปี
ผู้ป่วยชายไทยคู่ อายุ 35 ปี ลูกจ้างสังกัดกรุงเทพมหานคร จังหวัดกรุงเทพมหานคร
อาการสำคัญ มีอาการปวดท้องมากประมาณ 6 ชั่วโมง ก่อนมาโรงพยาบาล.
ประวัติปัจจุบัน 6 ชั่วโมง ก่อนมาโรงพยาบาลหลังจากกินเหล้า 3 ชั่วโมง ญาติสังเกตว่าผู้ป่วยมีอาการปวดท้องบริเวณลิ้นปี่ร่วมกับมีอาการเจ็บบริเวณอกทั้งสองข้าง หลังจากนั้นมีอาการหอบเหนื่อยหายใจเร็วหายใจลึก ปัสสาวะ อุจจาระปกติ ไม่มีประวัติคลื่นไส้ อาเจียน ไม่มีประวัติถ่ายดำ (ปกติหลังจากดื่มเหล้าผู้ป่วยจะเมาหลับ).
2 ชั่วโมง ก่อนมาโรงพยาบาล มารดาผู้ป่วยสังเกตว่าผู้ป่วยซึมลง หายใจยังคงเร็วและลึกจึงพามาโรงพยาบาล.


ภาพที่ 1-2. Bruise positive at lateral side of abdomen and downward to left thigh.
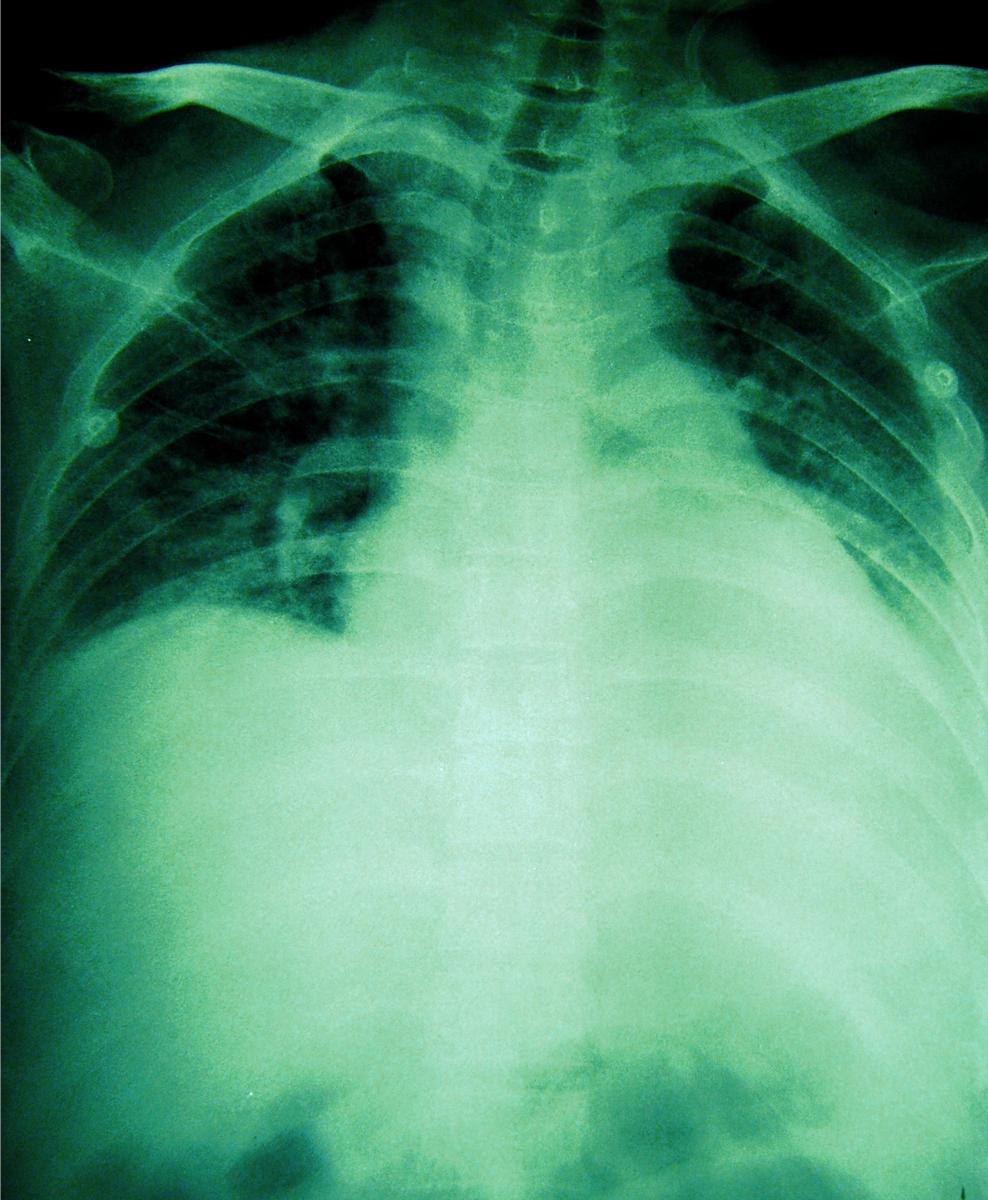
ภาพที่ 3. Chest X-ray วันแรกที่รับไว้ในโรงพยาบาล.

ภาพที่ 4. ให้การดูแลเรื่องอาการหอบเหนื่อยโดยใส่ท่อช่วยหายใจ
เพราะมี impending respiratory failure.


ภาพที่ 5-6. ผลการรักษาในผู้ป่วยรายนี้ได้ผลดี สามรถกลับบ้านได้ อาการบวมแดงที่ท้องและขาลด
ลง.
ประวัติอดีต
►ผู้ป่วยดื่มเหล้ามานาน 18 ปี (ตั้งแต่ปี พ.ศ. 2532) ดื่ม 2 กั๊ก/วัน ส่วนใหญ่ดื่มหลังกินข้าว เช้า-เย็น.
► ช่วง 2 ปีหลังนี้ดื่ม 3 กั๊ก/วัน ทุกวัน (หลังอาหารทุกมื้อ มื้อละกั๊ก สั่งจากร้านค้าข้างที่ทำงาน และร้านค้าใกล้บ้านมาดื่ม) ดื่มชนิด 40 ดีกรี.
► ไม่เคยคิดอยากเลิกเหล้ามาก่อน.
► ไม่เคยปวดท้อง/ถ่ายดำ/อาเจียนเป็นเลือดมาก่อน.
► รายได้ 8,800 บาท (ค่าเหล้า 3,000 บาท/เดือน) มีบุตร 2 คนเรียนอยู่ชั้น ม.3 และ ป.6.
► ภรรยาแยกกันอยู่เพราะทนเรื่องติดเหล้าไม่ได้.
ผลการตรวจร่างกาย
BT 38.0oC, RR 26/min, HR 102 /min, BP 80/50 mmHg.
A Thai male, mild pale conjunctive, no icteric sclera, drowsiness, look agitation due to dyspnea and Kussmaul breathing positive, non co-operative .
Heart : normal s1 s2 no murmur.
Lung : tachypnea, crepitation both lower lung, no decrease breath sounds.
Abdomen : active bowel sound (BS) generalized tenderness but decrease BS at epigastrium, hepatomegaly 3 FB. below RCM, liver span 13 cm, fist test negative, no splenomegaly, no ascites, bruise positive at lateral side of abdomen and downward to left thigh (ภาพที่ 1-2).
PR : no melena, normal sphincter tone, no rectal shelf.
Extremities : no pitting edema, swelling and inflammation found at left thigh.
Neurological exam : E3M6V5, drow siness, no flapping tremor, no frog legs
Motor grade 4 at least, BBK negative, Clonus negative, Sensory intact.
วิเคราะห์ปัญหาในผู้ป่วยรายนี้
ผู้ป่วยรายนี้มีปัญหาที่มาพบแพทย์ที่สำคัญที่สุด คือ อาการปวดท้องแบบเฉียบพลันที่เกิดร่วมกับอาการที่ซึมลง หายใจเร็วโดยมีประวัติการดื่มเหล้ามามากและนาน. ในส่วนของการตรวจร่างกายพบว่ามี hypotension, fever, dyspnea, Kussmaul breathing positive generalized abdominal tenderness with decrease BS. อาการทั้งหมดเป็นลักษณะที่กระทบต่อหลายระบบโดยมีอาการนำมาจากอาการปวดท้อง ทำให้ต้องคิดถึงสาเหตุที่อาจเป็นไปได้ ดังนี้
1. อวัยวะในช่องท้องที่มีการติดเชื้อร่วมกับมี การกระจายไปทุกระบบ (bacterial sepsis) โดยเฉพาะถ้าประเมินผู้ป่วยแล้วพบว่ามีภาวะตับแข็งร่วมด้วย.
2. อวัยวะที่น่าจะมีปัญหาเกี่ยวข้องจากเหล้าที่สำคัญก็คือ ตับอ่อนอักเสบ ที่แสดงอาการลักษณะของ SIR (systemic immune response).
ดังนั้นต้องมองหาสาเหตุดังกล่าวจากข้อมูลการตรวจเพิ่มเติม เช่น การทำ septic workup, film acute abdomen, chest X-ray, amylase, lipase, liver function test พร้อมกันกับการรีบให้การรักษาเบื้องต้นโดยเฉพาะการดูแลเรื่องอาการหอบเหนื่อยที่อาจมี respiratory failure, และการดูแลเรื่องสัญญาณชีพและ systemic immune response ให้คงตัวด้วย.
ผลการตรวจทางห้องปฏิบัติการและเอกซเรย์
CBC : Hb 7.7 g/dl, Hct 26.3 %, MCV 100, MCH 26.2, MCHC 29.3, RDW 23.6, WBC 45,000/มม.3, PMN 74%, L 21%, M 5%, platelet 492,000/มม.3
Arterial blood gas : pH 6.8, PCO2 12.1, PO2 121.3, HCO3 2.1, O2SAT 94.6%
Blood chemistry : FBS 374 mg/dl, BUN 17 mg/dl, Creatinine 1.10 mg/dl, Ca 8.2 mg/dl, Alb 3.7 gm/dl, TB 3.2 mg/dl, DB 1.7 mg/dl, SGOT 130 U/L, SGPT 28 U/L, Alk. phos 102 U/L, Amylase 379 mg/dl, Sodium 124 mEq/L, K 5.1 mEq/L, Chloride 84 mEq/L, Carbon dioxide 10, AGAP 25.1.
Prothrombin time 30.3 sec. (Normal 12.8 sec.), INR 2.3
APTT 84.6 sec (Normal 30.9 sec.)
URINE : Color Yellow, Blood 4+, Sp.gr. 1.020, pH 5.0, Protein 1+, Glucose 4+, WBC/HPF 0-1, RBC/HPF 2-3, Ketone positive.
Film chest X-ray : ดังแสดงในภาพที่ 3.
จากข้อมูลการตรวจเพิ่มเติมข้างต้นทำให้สนับสนุนสาเหตุที่ทำให้เกิดอาการทั้งหมดน่าจะมาจาก severe alcoholic pancreatitis metabolic acidosis; ketone นอกจากนี้ยังพบว่ามีภาวะเลือดจางและยังไม่มี หลักฐานที่ยืนยันว่ามีภาวะตับแข็งร่วมด้วย เนื่องจากร้อยละ 20 ของผู้ป่วยที่เกิดตับอ่อนอักเสบเฉียบพลันจะมีภาวะแทรกซ้อนที่รุนแรงได้แก่ การทำงานของอวัยวะต่างๆ ล้มเหลว, pancreatic necrosis, infected pancreatic necrosis และมีผลให้เกิดอัตราตายสูงถึงร้อยละ 10-30 โดยการเสียชีวิตจะเกิดในสัปดาห์ที่ 1-2 ประมาณร้อยละ 50 โดยมีสาเหตุการตายจาก renal failure, respiratory failure, GI. Bleeding, sepsis, severe acidosis, shock. ปัญหาในการดูแลผู้ป่วยกลุ่มนี้ จึงมีประเด็นที่ต้องให้ความสำคัญเพื่อ ลดอัตราตายและขณะเดียวกันก็จะช่วยบริหารจัดการความเสี่ยงในการดูแลปัญหานี้ได้อีกด้วย. จากการสำรวจข้อมูลการดูแลผู้ป่วยตับอ่อนอักเสบเฉียบพลัน ที่มีภาวะแทรกซ้อนที่รุนแรงในหลายประเทศของทางยุโรปพบว่า Ranson Score ยังคงเป็นที่นิยมใช้มากที่สุด มีการให้ antibiotic prophylaxis สูงถึงร้อยละ 73 และมีการเจาะเอาเนื้อเยื่อบริเวณ pancreatic necrosis มาทำการตรวจเพาะเชื้อเพียงร้อยละ 53 ดังนั้นจึงจำเป็นที่จะต้องประเมินความรุนแรงของตับอ่อนอักเสบเฉียบพลันก่อนและให้ความสำคัญของข้อมูลที่ได้เพื่อกำหนดแนวทางการรักษาที่จำเพาะกับผู้ป่วยต่อไป.
แนวทางการประเมินความรุนแรงของตับอ่อนอักเสบเฉียบพลันมีได้หลายวิธีแต่ที่มีใช้และน่าจะทำได้ง่าย เช่น ตรวจเลือดหาค่า C-reactive protein >= 150 มก./ดล. โดยตรวจได้ตั้งแต่แรกรับแต่จะมีความไวและแม่นยำที่สุดเมื่อทำซ้ำที่ 48 ชั่วโมง มีความแม่นยำและบ่งชี้การมี pancreatic necrosis ได้อีกด้วย หรือการทำ CT scan ได้ ก็คำนวณคะแนนตาม Balthazar CT severity index >= 4 หรือการพบว่ามี presence of pseudocyst or abscess ดังในตารางที่ 1. ส่วน Ranson Score สามารถใช้สำหรับประเมินความรุนแรงของตับอ่อนอักเสบเฉียบพลันจากเหล้าและนิ่วในถุงน้ำดีได้เช่นกัน.
การรรักษาเบื้องต้นในกรณี severe acute pancreatitis (SAP)
1. ให้การดูแลเรื่องอาการหอบเหนื่อยโดยใส่ท่อช่วยหายใจ เพราะมี impending respiratory failure ดังภาพที่ 4.
2. ให้การดูแลเรื่องสัญญาณชีพและ systemic immune response ให้คงตัวด้วย hydration, follow up hematocrit ไม่ให้มีลักษณะ Hemoconcentration และ arterial blood gas.
3. ประเมินผลความรุนแรงของโรคโดยการทำ CT scan เนื่องจากผู้ป่วยรายนี้มี organ failure ชัดเจนส่วนข้อบ่งชี้อื่นๆ เช่น อาการไม่ดีขึ้นหลังจากให้การรักษาประคับประคองไปแล้ว 48-72 ชั่วโมง ก็ควรทำการตรวจ CT scan โดยควรทำที่เวลาหลัง 72 ชั่วโมงไปแล้ว เพราะจะช่วยประเมินภาวะ pancreatic necrosis ได้ดีกว่ากรณีที่ทำ CT scan ตั้งแต่วันแรกๆ ส่วนในผู้ป่วยตับอ่อนอักเสบเฉียบพลันอื่นๆ ที่อาการไม่รุนแรงไม่จำเป็นต้องตรวจ CT scan เพราะสิ้นเปลืองและอาจไม่ช่วยในการรักษา.
4. พิจารณาให้ enteral feeding ทาง nasojejunal tube ในผู้ป่วย SAP ได้ตั้งแต่ระยะแรกเพราะมีความปลอดภัย สามารถลดอัตราการติดเชื้อลงได้ JPN Guidelines 2006.
5. Antibiotic prophylaxis ที่อาจช่วยลดการเกิด infected pancreatic necrosis ได้แต่ก็ยังมีข้อมูลขัดแย้งกันอยู่ ซึ่งต้องติดตามข้อมูลต่อไปดังภาพที่ 7.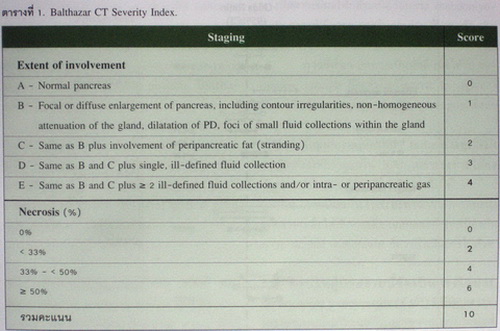
Blood chemistry : 2 วัน หลังรับไว้ในโรงพยาบาล
BUN 33 mg/dl, Creatinine 3.17 mg/dl, Ca 5.5 mg/dl, Alb 2.2 gm/dl, TB 1.44 mg/dl, DB 0.88 mg/dl, SGOT 220 U/L, SGPT 40 U/L, Alk 40 U/L, CPK 3837, LDH 1864 U/L, Lipase 1770 mg/dl, Mag 1.0 mg/dl.
Electrolyte : Sodium 129 mEq/L, K 4.2 mEq/L, Chloride 95 mEq/L, Carbon 20 mEq/L, AGAP 18.5.
Blood culture aerobic : No growth after 48 hours.
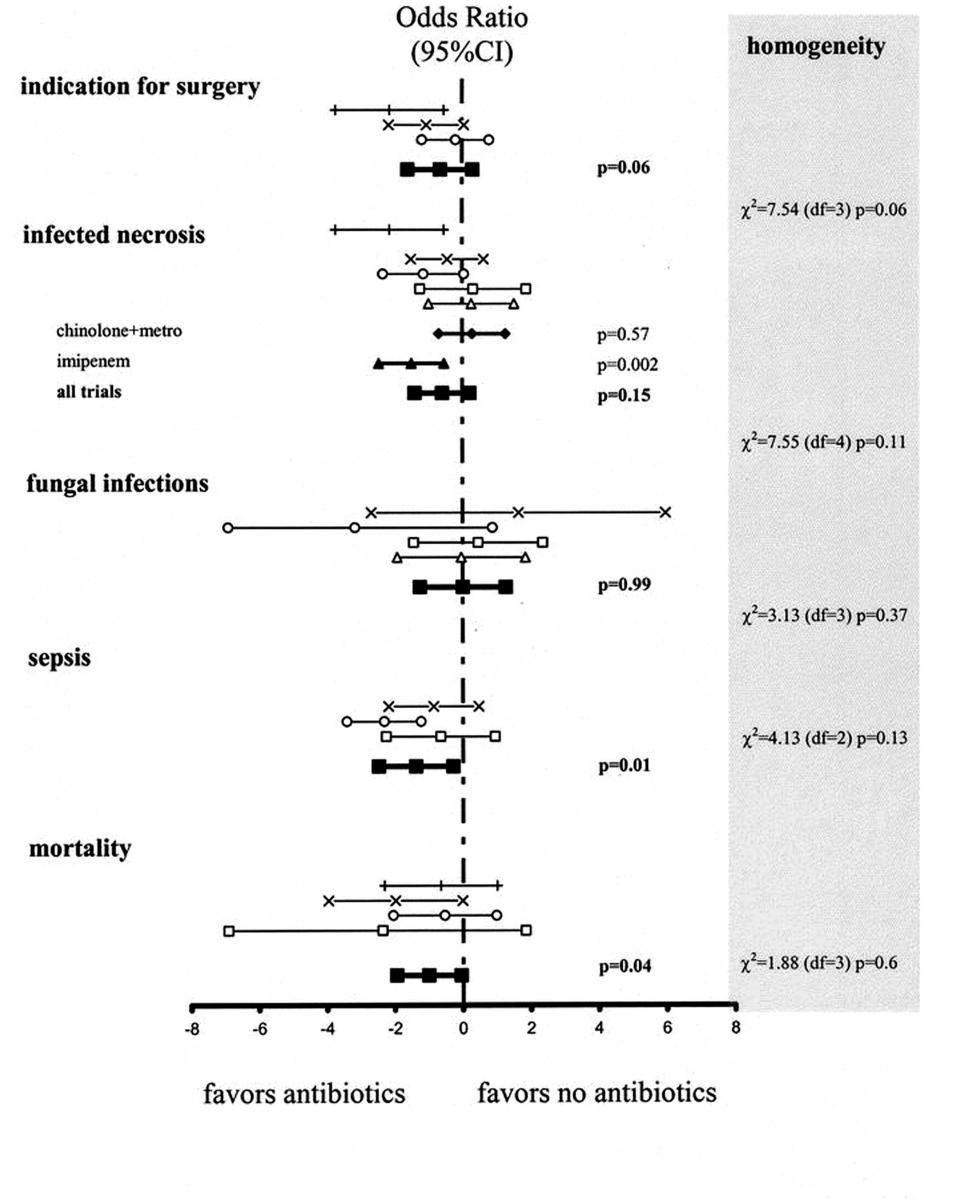
ภาพที่ 7. Antibiotic prophylaxis ที่อาจช่วยลดการเกิด infected pancreatic necrosis.
CT SCAN OF THE UPPER ABDOMEN: PANCREATIC PROTOCOL
♦ The liver is of normal size and parenchymal attenuation without space-taking lesion.
- There is no bile duct dilatation. The gallbladder is normally distended without demonstrable gallstone.
- There is no pancreatic duct dilata-tion or calcification. No non-enhanced are is observed.
- There is fluid in peripancreatic, anterior and posterior pararenal spaces. No cystic formation or collection is demonstrated. Moderate amount of ascites is also seen.
- The spleen, both kidneys and both adrenal glands are within normal limits.
- Retained NG tube is noted. The visualized bowel loops show mild dilatation with diffuse wall thickening and mucosal enhancement, as well as ascending colon. No pneumatosis intestinalis or portal vein gas is visualized. No free air is detected. The visualized SMA and SMV are also unremarkable.
- Diffuse stranding of mesenteric fat is noted, as well as subcutaneous fat.
- Bilateral pleural effusion with passive atelectasis of both basal lungs are seen.
- The bony structure appears unremarkable.
IMPRESSION : Prominent pancreas with diffusely heterogeneous enhancement, accompanying with fluid peripancreatic, anterior and posterior and posterior pararenal spaces, acute pancreatitis is possible, Balthazar CT scoring = 4.
Moderate ascites, Limited study of small bowel shows mild dilatation with diffuse wall thickening and mucosal enhancement, as well as ascending colon, ischemic bowel cannot be excluded. Bilateral pleural effusion with passive atelectasis.
การรักษาปัญหาตามระบบต่างๆ กรณี severe acute pancreatitis (SAP)
1. ปัญหาเกลือแร่ผิดปกติ จากกรณีที่มีอาการคลื่นไส้ อาเจียน และอดอาหาร ทำให้มีภาวะ ketoacidosis โดยมักเกิดร่วมกับภาวะ lactic acidosis และระดับน้ำตาลในเลือดต่ำ นอกจากนี้อาจมีระดับฟอสเฟตในเลือดลดต่ำลง และมีการสูญเสียแมกนีเซียมทางปัสสาวะเพิ่มขึ้นจากการการขับออก ทางปัสสาวะมีผลให้กล้ามเนื้ออ่อนแรง rhabdomyolysis ภาวะหัวใจวาย กระสับกระส่าย สับสน ชัก เกิดขึ้นได้.
การรักษา มักหายเป็นปกติ เมื่อได้รับ hydration, glucose ที่จะช่วยแก้ไขภาวะ hypoglycemia เพิ่มอัตราส่วนของ insulin/glucagon จึงลดการสร้าง ketoacid.
2. ปัญหา respiratory failure และ SIR จำเป็นต้องให้การดูแลใน ICU เพราะจะช่วยให้ลดปัญหาการประเมินผู้ป่วยที่ไม่เพียงพอไปได้.
3. การป้องกันในระยะยาว เช่น การแนะนำและช่วยเหลือให้เลิกการดื่มแอลกอฮอล์ การป้องกันภาวะ alcohol withdrawal ก็ควรดำเนินการไปด้วย.
สรุปในผู้ป่วยรายนี้จัดเป็นกรณีผู้ป่วย severe acute pancreatitis (SAP) ที่มีปัญหาต่อหลายระบบอันเป็นผลอันตรายจากแอลกอฮอล์ที่อาจทำให้เสียชีวิตได้ ผลการรักษาในผู้ป่วยรายนี้ได้ผลดี (ภาพที่ 5-6) แต่ก็จำเป็นต้องใช้ทรัพยากรที่สิ้นเปลืองมาก หากสามารถป้องกันได้ก็น่าจะเป็นประโยชน์ต่อทุกๆฝ่าย.
เอกสารอ้างอิง
1. King NK, Siriwardena AK. European survey of surgical strategies for the management of severe acute pancreatitis. Am J Gastroenterol 2004;99:719-28.
2. UK guidelines for the management of acute pancreatitis. Gut 2005;54 (Suppl 3):iii1-9.
3. Tsushima Y, Yamada S, Aoki J, et al. Effect of contrast-enhanced computed tomography on diagnosis and management of acute abdomen in adults. Clin Radiol 2002;57:507-13.
4. Rosen MP, Sands DZ, Longmaid III HE, et al. Impact of abdominal CT on the management of patients presenting to the emergency department with acute abdominal pain. Am J Roentgenol 2000;174:1391-6.
5. Balthazar EJ, Robinson DL, Megibow AJ, Ranson JH. Acute pancreatitis: value of CT in establishing prognosis. Radiology 1990;174:331-6.
6. Larvin M. Assessment of severity and prognosis in acute pancreatitis. Eur J Gastroenterol Hepatol 1997;9:122-30.
7. Takeda K, Takada T, Kawarada Y, et al. JPN Guidelines for the management of acute pancreatitis : medical management of acute pancreatitis. J Hepatobiliary Pancreat Surg 2006;13:42-7.
8. Wrenn KD, Slovis CM, Minion GE, Rutkowski R. The syndrome of alcoholic ketoacidosis. Am J Med 1991;91:119.
สมบัติ ตรีประเสริฐสุข พ.บ.
ผู้ช่วยศาสตราจารย์ คณะแพทยศาสตร์
จุฬาลงกรณ์มหาวิทยาลัย
- อ่าน 19,606 ครั้ง
 พิมพ์หน้านี้
พิมพ์หน้านี้